The Form
The Benefits Selction Form PDF from the MPI website.
This form must be filled out by all applicants!!
This form is where you declare which of the medical and dental plan options you wish to participate in. In this form, you must again list the dependents you will be including in your participation.
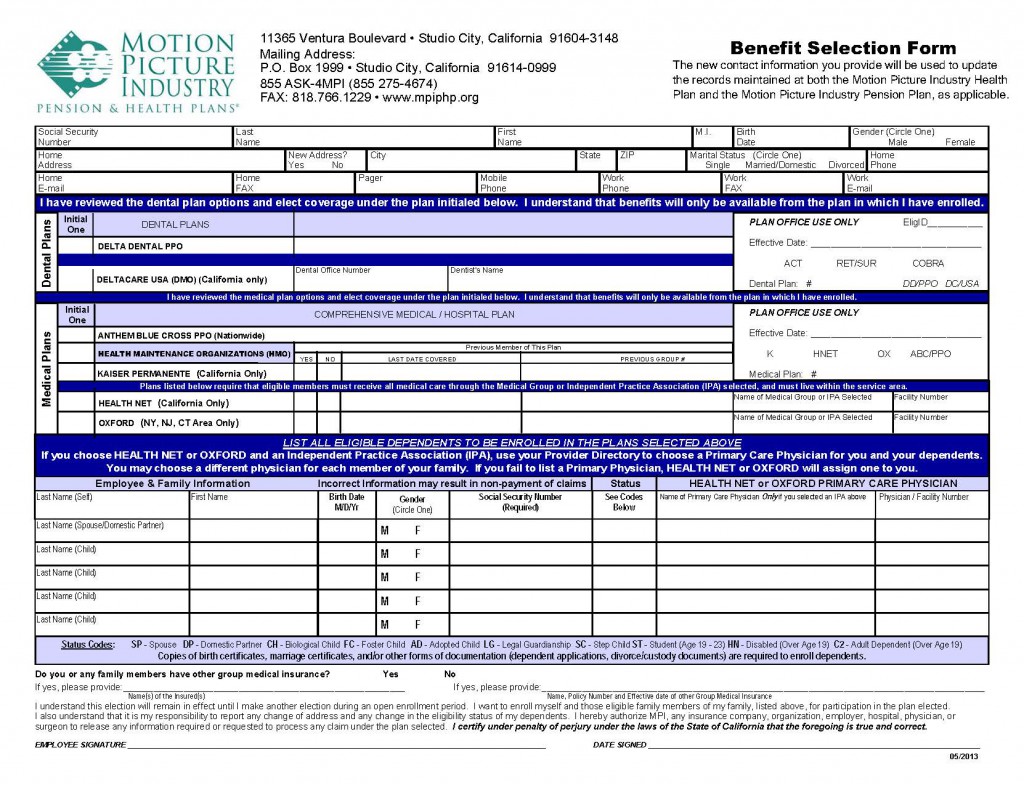
* Click the image for a larger view but access the form using the link above.
FIrst, fill out your information in the top section of the form above the purple line. Next, indicate which of the MPI Dental Plans you wish to participate in by putting your initials in the box next to the plan of your choice (Delta Dental PPO or Deltacare USA (Dental HMO)). In the next section, indicate which of the MPI Health Plan you wish to participate in by putting your initials in the box next to the plan of your choice. You can only choose between the Anthem Blue Cross, Kaiser Permanente or Health Net plans. The Oxford plan is not available for members in California.
In the bottom section of the form, everyone that you are interested including in your participation benefits needs to be listed in the appropriate rows. This includes your name and information. You will need to provide all participants names, birth dates, identify the person’s gender, list the person’s social security number, put the appropriate status code for each person based on the list under the section, and then list any previously identified primary care physicians, if you are going to participate in the HealthNet plan.
Be sure to sign and date the form at the bottom of the page before sending it to MPI.