The Form
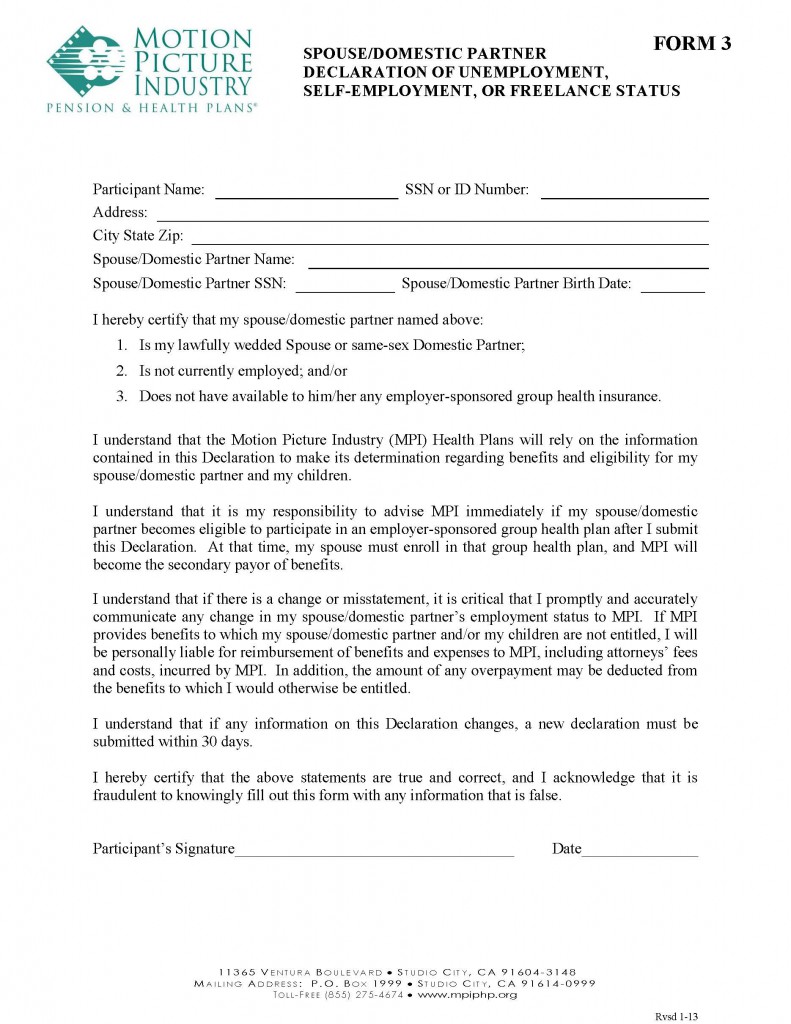
Form 3 – Employment Declaration from the MPI website.
This form must be filled out by those who want to cover their spouse or same-sex domestic partner in the MPI Health Plan
This form is only to be filled out if you want to add your spouse or same-sex domestic partner to your MPI Health Plan as a dependent, and they are either self-employed and have no insurance, or they are employed and their employer does not offer health insurance. If neither of the criteria apply, you do not need to return this form to MPI.
* Click the image for a larger view but access the form using the link above.
If you are providing this form because your spouse/partner meets the self-employed or no-health-insurance-offered-by-employer conditions, fill out the requested information at the top of the sheet. Be sure to sign and date the form at the bottom before returning to MPI.